- Barbaros Neighborhood, Sütçüyolu Street No:85/1, Ataşehir Istanbul
Laparoscopy Definition and Reasons for Performing
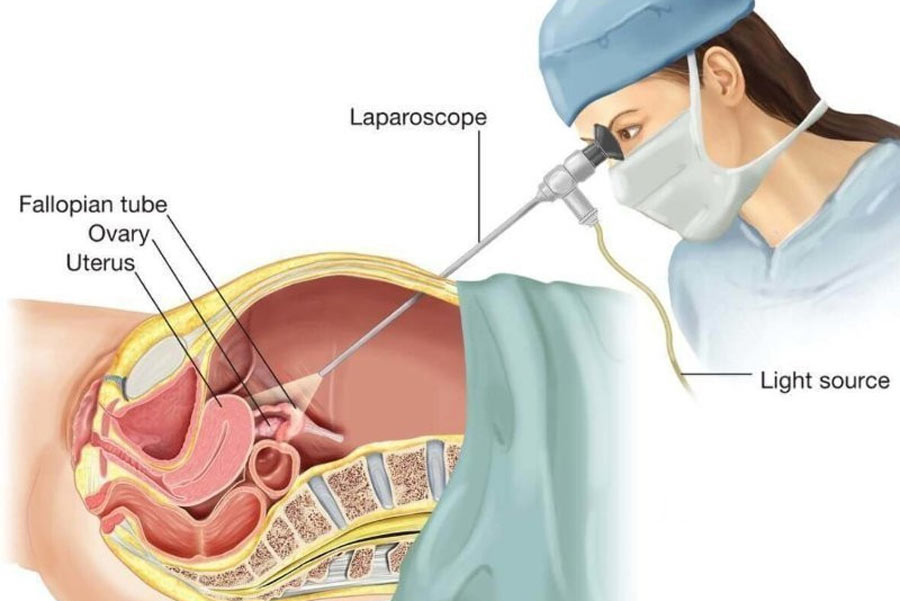
Laparoscopy is the name given to the process of observing the inside of the abdomen by means of an endoscope. In the past, laparoscopy was used only as a diagnostic tool, but today almost all gynecological operations can be performed with laparoscopy.
Who is eligible?
Laparoscopy is a suitable method for anyone whose general health condition is suitable for surgery. However, in patients with severe respiratory or heart problems, laparoscopy may not be preferred because the upside-down position is used during the procedure. In the presence of extreme obesity or previous abdominal surgeries (especially if they have been repeated more than once), laparoscopy may be difficult.
What are the advantages?
Most of the open surgeries performed today can now be performed with laparoscopy. The advantages of laparoscopy can be listed as follows;
1) It can usually be done on an outpatient basis;
2) The incisions on the skin are much smaller (0.5-1 cm) compared to other applications;
3) Less pain in the postoperative period;
4) It is faster to return to work and social life in the postoperative period.
The size of the operation performed inside is the same as open surgery.
What are Laparoscopic Applications?
Laparoscopic applications are divided into two as diagnostic and therapeutic or surgical laparoscopic applications.
Diagnostic Laparoscopy
Today, diagnostic laparoscopy has lost its value in the past and has become an increasingly preferred application. By definition, it is laparoscopy performed to reveal the cause of infertility in a woman who does not have any abnormalities in her history and examination.Severe menstrual pains that occur later in the history, pain during intercourse, pelvic surgery (removal of cysts or fibroids, removal of ectopic pregnancy, etc.), sexually transmitted infections (gonorrhea, chlamydia, pelvic inflammatory diseases, etc.), examination and ultrasound findings in a woman who does not have intrauterine device use, and if the uterine film (HSG) is in normal condition, there will be no significant disease that can be seen when laparoscopy is performed. In this case, there is a possibility of mild endometriosis, mild adhesions or obstruction in the tubes in laparoscopy. It is very rare for the tubes to be blocked in laparoscopy in a woman whose tubes are open in the uterine film and it usually occurs due to a contraction (spasm) in the tubes during the procedure. The extent to which mild adhesions and mild endometriosis are the cause of infertility and to what extent the treatment is beneficial is a subject that needs to be discussed.In cases where these findings are seen, the treatment is the same as in unexplained infertility.
Surgical laparoscopy
It is the name given to laparoscopic applications performed for the treatment of a disease detected using examination and imaging techniques or for the removal of the diseased organ.
Laparoscopic applications performed to increase conception
(Adhesiolysis-adhesion opening; salpingostomy-opening of the fully closed tube and fimbrioplasty-opening of the partially closed tube):
Previous infections, surgical operations, previous apendecitis or endometriosis can often lead to adhesions that disrupt the relationship between the tube and the ovary. If the adhesions are thin and technically openable, laparoscopic adhesion opening called adhesion can be beneficial. After the restoration of the normal anatomical relationship between the tube and the ovaries, pregnancy rates between 30-60% have been reported within 1 year, depending on the age of the woman and whether there are additional infertility factors. In cases where adhesions are seen intensely, pregnancy rates are at a low level as there is a high probability of re-adhesion after opening. There is also a possibility that the tubes that are closed during laparoscopy will be opened. Tubes (hydrosalpinx), which are especially blocked from the part that opens into the abdominal cavity (the end adjacent to the ovary), can be opened with a procedure called salpingostomy. If this obstruction is partial, not complete, opening can be achieved (fimbrioplasty). Depending on the damage to the inner layer of the tube, the thickness of the wall of the tube and the presence of surrounding adhesions, reclosure rates vary between 30-100% and pregnancy rates vary between 10-70%. In cases where it is not possible to open the tubes, the tubes should be removed as a preparation for the subsequent IVF application. Leaving the clogged tubes in place has a negative effect on the pregnancy rates in IVF
Laparoscopic endometriosis surgery (Endometriosis)
One of the diseases in which laparoscopy is most often used is endometriosis. Endometriosis disease occurs when the cells lining the uterus settle and reproduce outside the uterus. The disease most commonly involves the peritoneum and ovaries, called the peritoneum. It also settles in the area between the uterus and the large intestine, causing painful lesions. In its advanced stages, it attaches the uterus, tubes, ovaries, and intestines together, causing pain, infertility, and mass symptoms. In the early stage of the disease, there are lesions on the peritoneum in the form of gunpowder burns. These lesions can be removed by burning during laparoscopy or by vaporizing with a laser.
It is possible to remove endometriosis lesions, called deep endometriosis, which involve the area between the uterus and the intestine, laparoscopically. Pain is usually relieved by removing these lesions. Advanced endometriosis surgery is a long-term treatment that requires the presence of an experienced surgeon. It should not be forgotten that endometriosis is a disease with a risk of recurrence. Women have a 30-50% risk of recurrence, especially in their pre-menopausal lives. For this reason, we recommend in vitro fertilization in women who want to have children if there is no pregnancy within 6-12 months following an operation in which all endometriosis lesions are removed. Vaccination treatments are often not recommended because they are usually associated with a low pregnancy rate.
Laparoscopic cyst surgery
Although endometriomas are the most common cysts that are intervened with laparoscopy, laparoscopic intervention may also be required in simple cysts and dermoid cysts that persist and do not regress
In more advanced stages, cystic structures called endometriomas form in the ovaries. With laparoscopic removal of endometriosis cysts, the chance of pregnancy in infertile couples increases. It is very important that laparoscopy is performed carefully so as not to damage the ovarian capacity. During the peeling of the endometrioma cyst capsule, there is a possibility that the normal ovarian tissue will not be damaged and there will be a decrease in ovarian capacity. Both the endometriosis itself and the intervention can inevitably lead to a decrease in ovarian reserve. For this reason, in recent years, especially in women with recurrent cysts, in vitro fertilization is preferred if there is a desire to have a child rather than re-surgery. ,
Dermoid cysts: Dermoid cysts are cysts that contain parts of all tissues of the body. These can include fat, hair, teeth, nerves and muscle tissue. They usually occur as a result of these cells being trapped in the ovary before birth. For what reason they grow is unknown. Dermoid cysts most often cause a complication called torsion. Torsion is the rotation of the ovary around its own axis with the adjacent tube and as a result, the deterioration of blood supply. If not intervened laparoscopically in time, necrosis occurs in the ovaries and tubes and they must be removed. Dermoid cysts should be removed, especially after they reach a diameter of 3-4 cm. They are quite easy to remove laparoscopically. Since 15% of women may have dermoid cysts in both ovaries, the ovary, which seems to be intact, should also be carefully examined. Dermoid cysts have a 1% probability of being malignant. Malignant ones have immature nerve tissues inside.
Paraovarian cysts: They are cysts that develop from congenital residues in the neighborhood of the ovary. Rarely, they have the potential to be malignant. When they reach large sizes, they need to be taken. They are easy to remove laparoscopically.
Cystadenomas: They are tumors that develop in the ovary and have the potential to be malignant. It is suspected by monitoring liquid and solid structures together on ultrasound and the definitive diagnosis is made by removing the cyst. Serous and mucinous cystadenomas are the most common. They are easy to remove laparoscopically. In women who are close to menopause, the removal of the ovary is a more correct procedure. In younger women, only cysts can be removed, but a pathological examination (frozen section) should be performed during the operation and it should be evaluated whether they are malignant or not.
Laparoscopic Myoma Surgery
A significant part of fibroids can be removed laparoscopically. The indications for operation in fibroids are as follows:
Size: It is generally recommended to remove fibroids that have exceeded 6 cm and fibroids that have recently grown rapidly.
Bleeding: Fibroids do not cause bleeding unless they enter the inner layer of the uterus (endometrium) or compress. If there is bleeding in the mions that have entered the uterus, surgery is recommended regardless of their size. The surgical intervention to be performed here is hysteroscopic myomectomy, that is, the myoma is removed by hysteroscopy by entering from below.
Compression complaints: When fibroids are in a position called intraligamentary, they can put pressure on the ducts that bring urine from the kidneys to the bladder, called ureters. A fibroid in this position should be removed when it gives pressure symptoms. Fibroids that develop in front of the uterus can put pressure on the bladder, and fibroids that develop in the back can put pressure on the rectum.
Infertility: Fibroids are usually not the cause of infertility. However, if there is no reason to explain infertility in the researches, they may need to be removed. Generally, it is recommended to take those that are 4 cm and above. If there is a fibroid that enters the uterus and the couple cannot get pregnant, it is recommended to remove them regardless of whether there are any other complaints and the size of the fibroids.
It is preferred that fibroids that are suitable for laparoscopic removal are smaller than 8 cm in size, those larger than 3 cm are 3 or less in total number and are not deeply embedded in the uterine wall. After the fibroids are removed laparoscopically, pregnancy is not allowed for a few months. Laparoscopic fibroid surgery may take 1-3 hours depending on the size and location of the fibroids. The patient usually stays in the hospital for 1 day and is discharged the next day.
Laparoscopic Hysterectomy
Removal of the uterus is possible laparoscopically. In cases of uterine prolapse, the preferred is the removal of the uterus from the vagina (vaginal hysterectomy). Laparoscopic hysterectomy is an alternative to hysterectomy performed by opening the abdomen, and a uterus that can be removed vaginally should not be removed laparoscopically. Laparoscopic hysterectomy is a successful operation in experienced hands and carries all the advantages of laparoscopy. After part of the uterus is released laparoscopically, it is removed vaginally. The patient stays in the hospital for 1-2 days and is discharged
